Overview and history
Mifepristone was developed during the early 1980s by researchers at the French pharmaceutical company Roussel Uclaf. While investigating glucocorticoid receptor antagonists, investigators discovered that some of the compounds blocked the similarly shaped progesterone receptor. Refinement of the compound led to the production of RU486, the medication now known as mifepristone.
Clinical testing of mifepristone began in Europe in 1982. The results from the clinical trials showed that mifepristone, when used alone, induced a complete abortion in 60% of women with pregnancies up to 49 days' gestation. Investigators then discovered that by adding small doses of a prostaglandin analog on the last day of mifepristone treatment, the complete abortion rate increased to over 95%. France became the first country to license the mifepristone/prostaglandin analog regimen for early abortion in 1988.
Mifepristone worldwide
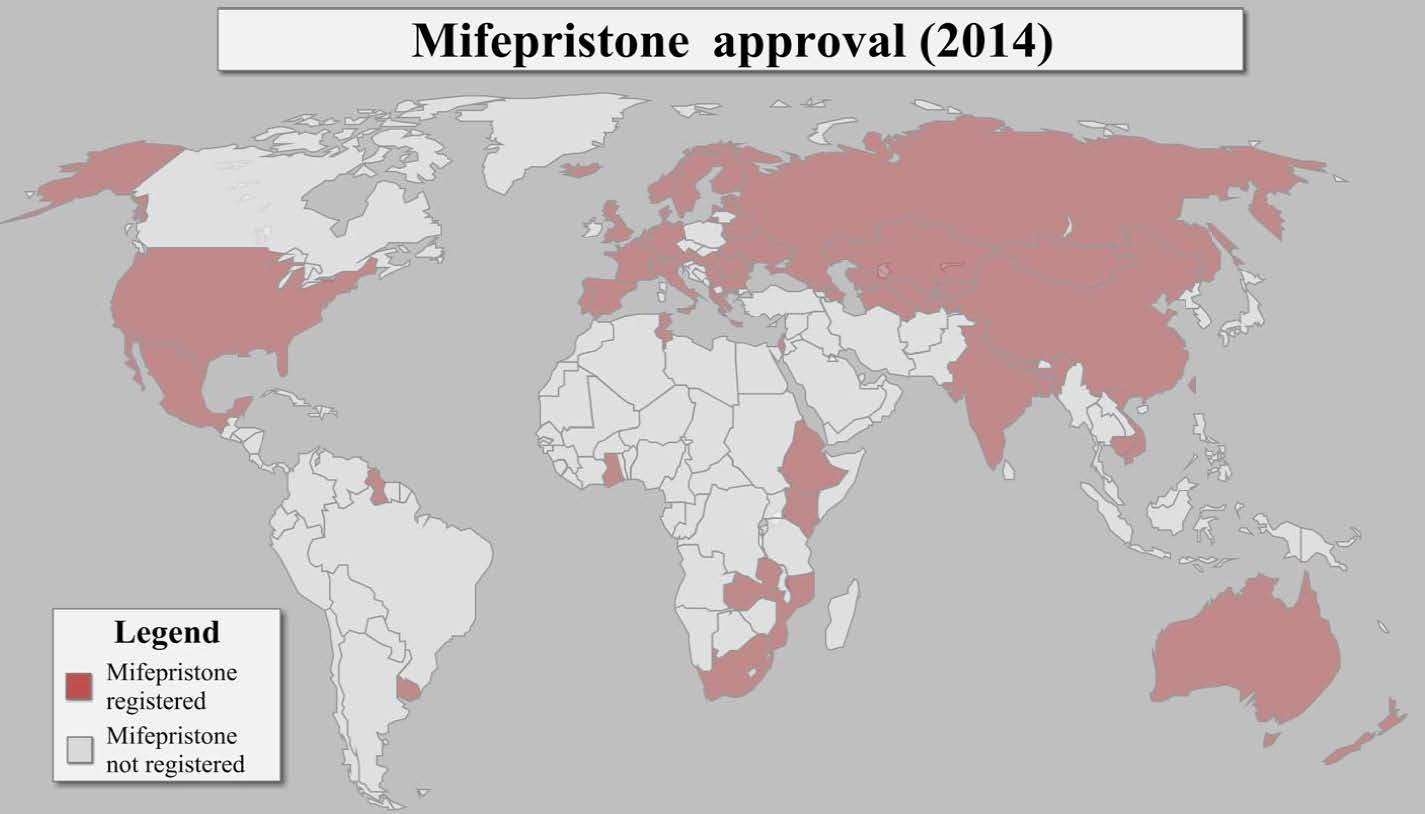
Since 1988, Mifepristone has been registered for medication abortion use in nearly 60 other countries worldwide. Worldwide tens of millions of women have used mifepristone and a prostaglandin analog to terminate pregnancy with impressive safety and efficacy. Mifepristone is sold under a number of different brand names around the world, including Mifegyne, Mifebort, and Termipil. In some countries, mifepristone and misoprostol are available in a combination package (such as Medabon). Mifepristone may also be available in additional countries through the black market. In unregulated markets, the quality of mifepristone may vary and thus the reliability of the source should be examined. >
Mifepristone in the US
In September 2000, the US Food and Drug Administration (FDA) approved the use of mifepristone in combination with misoprostol for early pregnancy termination. Since the approval of the mifepristone/misoprostol regimen, medication abortion has become an integral component of abortion care in the US. Over one million women in the US have used mifepristone/misoprostol to terminate a pregnancy and the method accounts for approximately one in five early abortions. The number of abortion providers offering medication abortion also has steadily increased. In the US, the brand names of mifepristone and misoprostol are Mifeprex and Cytotec, respectively.
Mechanism of action of mifepristone
Mifepristone (a synthetic steroid) is an anti-progestin that blocks the action of progesterone, a hormone necessary to maintain a pregnancy. By blocking the action of progesterone, mifepristone alters the endometrium (the uterine lining), induces menstrual bleeding, and causes the uterine lining to shed. Mifepristone also causes the cervix to soften and initiates uterine contractions.
Mifepristone is used in conjunction with misoprostol. Misoprostol is an analog of prostaglandin E1. By interacting with prostaglandin receptors, misoprostol causes the cervix to soften and the uterus to contract, resulting in the expulsion of the uterine contents.
Evidence-based mifepristone and misoprostol regimen
A number of different protocols have been approved worldwide. A significant amount of research has been conducted in a variety of countries and the results of have demonstrated that a number of protocols are equally effective. The a synthesis of these protocols and the outcomes of various clinical trials indicates that the mifepristone/misoprostol regimen can be used with very high efficacy through nine weeks’ gestation when 200mg of mifepristone is administered orally and is then followed with 400 to 800 micrograms of misoprostol 24-48 hours later. The misoprostol can be administered buccally (in the cheek), sublingually (under the tongue), or vaginally. A growing body of research indicates that both medications can be taken from home, timed to a woman’s particular life circumstances. However, many countries regulate the process such that mifepristone (and sometimes misoprostol) must be taken in a clinic.
A follow-up visit with a health service provider 1-2 weeks after the abortion is often recommended. However, studies have also called into question the need for a routine, in-person post-abortion. Results from a mifepristone/misoprostol clinical trial conducted in China, Cuba, and India suggest that women who experience an incomplete abortion are able to identify their condition correctly. Investigation into possible alternatives to universal in-person follow-up, such as telephone follow-up with home pregnancy testing and in-person follow-up for selected patients, is ongoing. In the last few years, research has demonstrated that women can use mifepristone/misoprostol through telemedicine models of service delivery.
Regardless of which protocol is used, there are several steps involved in obtaining a medication abortion with mifepristone/misoprostol.
- Step I: A trained provider counsels the woman, takes a medical history, and ascertains gestational age. Accurate dating of the pregnancy is important and can occur through either clinical assessment or ultrasound. If the woman is eligible for a medication abortion using mifepristone/misoprostol she takes mifepristone orally. Pain medication is commonly prescribed at this time, in case the woman needs it later.
- Step II: One or two days after taking mifepristone, the woman takes misoprostol to complete the abortion. This can be taken at home or in the clinic, depending on the protocol. In some cases, a woman may abort after the mifepristone alone.
- Step III: Several to fifteen days later, the woman confirms that the abortion is complete. This can be based on her own assessment (often with the aid of a symptom checklist and a home pregnancy test) or presentation at a clinic. Studies have confirmed that women are generally able to accurately assess when follow-up with a provider is necessary. Completion is often clinically evident, but sometimes an ultrasound is necessary for confirmation. The only ultrasound finding which reliably demonstrates incompletion is the presence of a persistent gestational sac. If the abortion is not complete, the clinician will discuss treatment options with the woman. These options may include waiting and reevaluating for a complete abortion, administering additional misoprostol, or performing a vacuum aspiration to empty the uterus.
Efficacy
Numerous studies have now overwhelmingly demonstrated the efficacy and safety of the mifepristone/misoprostol regimen. Approximately 95%-98% of women will have a successful abortion when using mifepristone/misoprostol within nine weeks from the onset of the last menstrual period. Medication abortion completion rates are at the higher end of this range at earlier gestational ages. Recent evidence suggests that the mifepristone/misoprostol regimen continues to work beyond nine weeks, but efficacy decreases.
With respect to the timing of the abortion, approximately, 67% of women will have a complete abortion within four hours of using misoprostol and approximately 90% of women will have a complete abortion within 24 hours of using misoprostol. For women who do not experience a complete abortion an aspiration intervention may be required. Reasons for an aspiration intervention include prolonged or excessive bleeding, incomplete abortion (remnants of fetal tissue in the uterus), or an ongoing pregnancy. An aspiration termination may also be performed at the request of the woman or the provider. Ongoing pregnancy occurs in fewer than 1% of cases.
Eligibility
Most women with an unwanted pregnancy of up through 63 days' gestation can use the mifepristone/misoprostol regimen. If the use of mifepristone/misoprostol does not result in a complete abortion, aspiration intervention may be necessary. Women considering the mifepristone/misoprostol regimen should be willing to undergo an aspiration procedure, if indicated.
Contraindications
Women with a confirmed or suspected ectopic (extra-uterine) pregnancy, a history of allergy to either mifepristone or misoprostol, chronic systemic use of corticosteroids, chronic adrenal failure, coagulopathy or current therapy with anticoagulants, and/or inherited porphyria are contraindicated from using the mifepristone/misoprostol regimen. Further, if an intrauterine device (IUD) is present, the device must be removed before the medication abortion is initiated. In addition, women with chronic medical conditions, including hypertension, severe hepatic or renal disease, and severe anemia, should be evaluated individually.
Effects, side effects, and complications
Effects
Abdominal cramping and vaginal bleeding are hallmarks of the abortion process. Many women and clinicians report cramps and abdominal pain similar to those associated with a heavy menstrual period or a spontaneous miscarriage. Women also describe the Vaginal bleeding can vary significantly in both duration and severity. One study of mifepristone used with a vaginal prostaglandin to treat women through 63 days' gestation found that median blood loss was about 75ml, compared with 50ml typically lost during menses. Light bleeding and spotting can last for 1-3 weeks with a median for 9-13 days. The heaviest period of bleeding typically occurs when the products of conception are being expelled and persists for 1-4 hours.
Side effects
Side effects of the medications include nausea, vomiting, diarrhea, fever, and chills. In most cases, side effects can be managed with appropriate counseling and symptomatic treatments, such as oral analgesics for pain. Temperature elevation (defined as more than 100.4°F or 38°C) that is sustained (more than four hours) or begins more than 6 to 8 hours after misoprostol administration warrants clinical assessment.
To date, there is no evidence that mifepristone has teratogenic effects on the fetus. Several case reports have associated misoprostol use with limb defects and Mobius syndrome. However, an absolute causal relationship between misoprostol use and fetal deformities has yet to be demonstrated through prospective trials.
Complications
On rare occasion, uterine bleeding can be extremely heavy or prolonged. Approximately 1% of women experience uterine bleeding that requires vacuum aspiration and about 0.1% require transfusion. Less than 1% experience ongoing pregnancy. In 2% to 5% of cases the medication abortion is incomplete. Patients may require vacuum aspiration to resolve an incomplete abortion, end a continuing pregnancy, or control bleeding.
Acceptability
Studies in the US, Europe, Asia, Latin America, and the Middle East have demonstrated high rates of acceptability among patients using the mifepristone/misoprostol regimen. More than 90% of women in most studies reported being satisfied with the regimen. Several studies have found that more than 85% of women would choose the regimen again as well as recommend the regimen to a friend. Even among women who experienced an incomplete abortion, more than two thirds reported that they would use the regimen again.
Women consistently report that the best features of the mifepristone/misoprostol regimen include:
- The ability to avoid surgery and anesthesia;
- The perception that the process is more "natural";
- The perception of privacy; and
- The convenience
Women also consistently report that the least liked features of the process include:
- Length and degree of bleeding;
- Number of clinic visits; and
- Uncertainty as to whether or not the procedure had resulted in a complete abortion
Additional uses of mifepristone
Research is currently underway to study other beneficial uses of mifepristone. Issues under investigation include the use of mifepristone in labor induction, infertility treatment, and fibroid and meningioma tumors treatment. Studies have also shown that mifepristone when used in low doses serves as an effective post-coital contraceptive method.
For a list of sources consulted for this section of the website, please visit our reference section.