Overview and history
Despite evidence demonstrating the safety and efficacy of the mifepristone/misoprostol regimen, political and commercial difficulties present challenges to widespread production and distribution of mifepristone. Beginning in the early 1990s, researchers revisited the possibility of using misoprostol alone as a method of terminating early pregnancies. A considerable body of evidence has now shown that misoprostol can be used as a single agent to induce an early abortion. Misoprostol is inexpensive, stable at ambient temperatures, easy to transport, easy to administer, and does not require refrigeration, even in hot climates. Thus misoprostol has the potential to significantly expand medication abortion access in developing countries and low resources settings.
In recent years, misoprostol has been added to the World Health Organization’s List of Essential Medicines for incomplete abortion management and post-partum hemorrhage prevention. This has led to a number of efforts to increase community-based distribution of and widespread access to misoprostol, particularly in low resource settings. However, due to its use as an abortifacient, some governments have restricted or attempted to restrict access to and use of misoprostol. As a result, the availability and cost of misoprostol may vary widely, even in countries that have approved misoprostol for one or more indications. Misoprostol may be available in countries in which it has not been formally approved, typically through the black market or from community pharmacies or drug shops. The misoprostol available through unregulated markets may be of variable quality and cost.
Because misoprostol is widely available, generally inexpensive, and stable at room temperature, misoprostol is a suitable abortifacient in low-resource settings, particularly when more effective alternatives are not available. Over the last decade there have also been a number of efforts to expand access to misoprostol in settings were abortion is severely legally restricted and safe services are limited in order to reduce harm from unsafe abortion practices.
Misoprostol-only
experience worldwide
Many women, particularly in countries and settings with restrictive abortion laws, attempt to terminate early pregnancies with misoprostol alone. Reports from Latin America suggest that women frequently use misoprostol to induce abortion early in pregnancy. However, without standardized information and instructions, women utilize misoprostol in a numerous ways, with a high degree of variation in both dosage and timing. Some of these regimens are not as effective as others. Providing both health service providers and individual women with information about the evidence-based regimen for misoprostol use is critical.
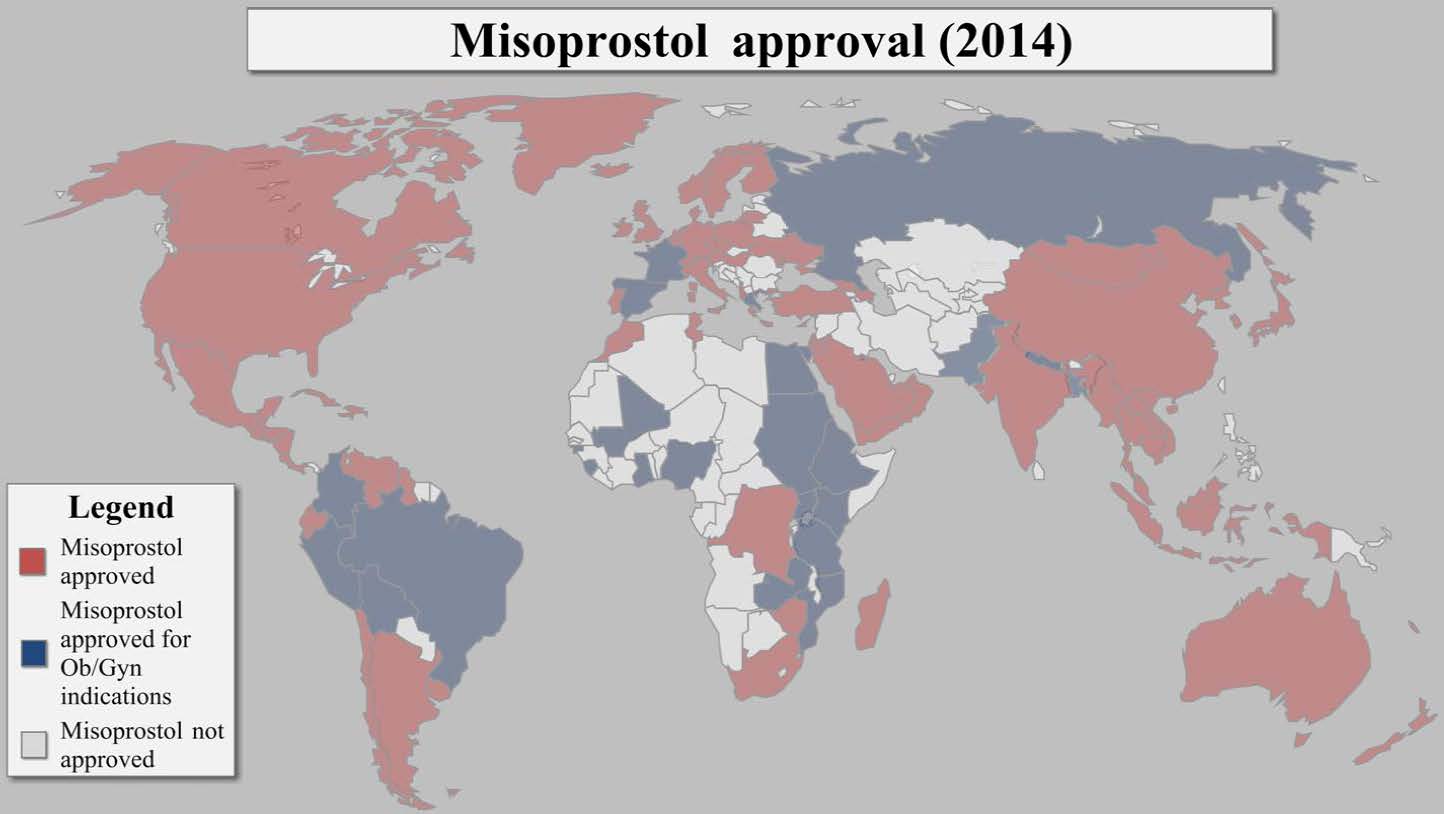
As indicated on the map below, misoprostol is currently registered in over 100 countries worldwide. In most countries, misoprostol has been approved specifically for use in the prevention non-steroidal anti-inflammatory drug-induced gastric ulcers. However, misoprostol is often used "off label" for its many obstetric and gynecological indications. In an increasing number of countries, misoprostol has been approved specifically for Ob/Gyn indications, including post-partum hemorrhage prevention, incomplete abortion management, and, in conjunction with mifepristone, early pregnancy termination.
Misoprostol-only experience in the US
In the US, misoprostol (brand name Cytotec®) has been approved by the US Food and Drug Administration (FDA) only for the prevention and treatment of gastric ulcers. However, clinicians routinely use misoprostol off-label for obstetric and gynecological purposes, including cervical ripening and labor induction. Further, the FDA has approved the use of misoprostol in conjunction with mifepristone for the termination of early pregnancies.
Misoprostol-only regimens are not widely used in the US, where mifepristone and misoprostol, methotrexate and misoprostol, and aspiration abortion services are available. However, the off-label use of misoprostol as a single agent abortifacient has been documented, particularly among Latinas in the US. Further, as state-level restrictions have created significant barriers to accessing clinic-based abortion care, in recent years there has been a reported increased in self-induction with misoprostol in certain regions of the country.
Mechanism of action of misoprostol
Prostaglandins are naturally occurring fatty acids produced by many tissues in the body. Prostaglandin E1 causes myometrial contractions by interacting with specific receptors on myometrial cells. This interaction results in a cascade of events, including a change in calcium concentration, thereby initiating muscle contraction. Misoprostol is an analog of prostaglandin E1. By interacting with prostaglandin receptors, misoprostol causes the cervix to soften and the uterus to contract, resulting in the expulsion of the uterine contents. Misoprostol is relatively metabolically resistant and thus has prolonged action. Misoprostol is absorbed through mucosal surfaces and thus can be administered through a number of different routes.
Misoprostol-only protocol
Determining the optimal protocol for the use of misoprostol as a single agent abortifacient has been an active area of investigation. Researchers throughout Latin America and Asia have explored buccal, sublingual, and vaginal regimens, a variety of doses, and different dosing schedules. Overall, these studies have shown that misoprostol alone can be effectively used in different clinical environments, at different doses, and through different routes of administration.
The results of these studies have informed the development of a consensus regimen for the use of misoprostol for the termination of an early pregnancy. The optimal regimen for pregnancies through nine weeks’ gestation is 800 micrograms of misoprostol followed 3-12 hours later with a second 800 micrograms of misoprostol followed 3-12 hours later by a third 800 microgram dose (3 doses x 800micrograms). These doses can be administered buccally (between the cheek and the gum), sublingually (under the tongue), or vaginally with equal efficacy. Importantly, all three doses should be administered the same way. If the woman uses the buccal or sub-lingual regimen, she should keep the pills in place for 30 minutes at which point she can swallow any pill remnants.
However, there are other protocols that appear to be as effective. This includes the vaginal administration of 800 micrograms followed 24 hours later by a second dose of 800 micrograms administered vaginally. There is some evidence that the efficacy of this regimen can be enhanced if the misoprostol tablets are moistened with a few drops of clean water prior to vaginal insertion.
Efficacy
The best available evidence suggests that the optimal protocol has an overall completion rate of 75% to 85% when used in the first nine weeks of pregnancy. Efficacy appears to be at the higher end of this range when the pregnancy is at an earlier gestational age. In the roughly 15%-25% of cases where misoprostol administration does not lead to a complete abortion, additional intervention in required. Recent studies have shown that approximately 10% of women using misoprostol for early pregnancy termination will experience an ongoing pregnancy. A woman may take an additional 800 microgram dose of misoprostol or she may need an aspiration intervention. Reasons for aspiration intervention include prolonged or excessive bleeding, incomplete abortion (remnants of fetal tissue in the uterus), or an ongoing pregnancy. An aspiration termination may also be performed at the request of the woman or the provider.
The misoprostol-only regimen has the potential to expand access to safe abortion services in resource poor and developing country settings. However, the misoprostol-only regimen is not as effective as either the mifepristone/misoprostol or the methotrexate/misoprostol regimen. Further, the side effects associated with the misoprostol-only regimen, while tolerable, are generally more severe than those associated with the combined regimens.
Eligibility
Most women early in their pregnancies appear to be eligible for the misoprostol-only regimen. If the use of misoprostol-only results in an incomplete abortion or a continued pregnancy, an aspiration abortion may be necessary. Women considering the misoprostol-only regimen should we willing and able to undergo an instrument aspiration procedure, if indicated.
Contraindications
Few contraindications to misoprostol use are described in the medical literature and most women with an intra-uterine pregnancy of nine weeks or less are eligible for misoprostol use. If a woman has a documented allergy to prostaglandins, in general, or misoprostol specifically, she should not use misoprostol. If an ectopic pregnancy is confirmed or strongly suspected, the woman should not use misoprostol. Finally, if a woman has an intrauterine device (IUD) in her uterus (an IUD in situ), the device should be removed before the administration of misoprostol.
Women with uterine infections, severe anemia, cardiovascular and cerebrovascular diseases, coagulopathy or current therapy with anticoagulants, and hypertension were excluded from some clinical studies. In these cases, use of misoprostol should be evaluated on a case by case basis.
Effects, side effects, and complications
Effects
Abdominal cramping and bleeding are hallmarks of the abortion process itself. Many women report that cramps and abdominal pain are similar to those associated with a heavy menstrual period. Vaginal bleeding can vary significantly in both duration and severity and many women report that the bleeding resembles a very heavy period or an early miscarriage. The majority of studies conducted on the misoprostol-only regimen have reported that the mean duration of bleeding is approximately two weeks. Many women report passing blood clots, which can be large, and some women report passing gray or tan tissue (the products of conception). This tissue is usually less than one or two inches in length.
Side effects
Reported side effects include nausea, vomiting, diarrhea, dizziness, headache, fever, chills, rashes, and pelvic pain. In most cases, these side effects are transient and resolve within 24 hours of misoprostol administration. Of women who report pelvic pain after using the misoprostol-only regimen, approximately 25% report that the pain was much stronger than menstrual pain. In most cases, side effects and pelvic pain can be managed with oral pain medications (like ibu profren).
A number of case reports from Brazil have associated fetal exposure to misoprostol with an increased risk of limb and central nervous system abnormalities. However, the absolute risk associated with in utero misoprostol exposure appears low. Women electing to use the misoprostol-only regimen should be informed of the possible teratogenic effects of misoprostol that may occur if the medication fails to induce an abortion and if the pregnancy is then carried to term.
Complications
Serious complications after misoprostol use are relatively rare. However, the woman should contact a provider if:
1) She experiences fever or chills beyond 24 hours after misoprostol administration;
2) She soaks more than two large maxi pads (or thick towels) an hour for two consecutive hours or if she experiences continuous bleeding for several weeks;
3) She experiences an abrupt onset of heavy bleeding two weeks or more after having taken misoprostol; and/or
4) She has no or scant bleeding in the seven days after misoprostol administration.
In approximately 15%-20% of cases, the abortion is incomplete and either an additional dose of misoprostol or an aspiration intervention is required. As use of misoprostol leads to cervical dilation, mechanical dilation is generally unnecessary if an aspiration abortion is performed.
Acceptability
Few studies have directly assessed the acceptability of misoprostol-only regimens. Although side effects of greater severity are associated with the misoprostol-only regimen, the majority of patients report that the side effects are tolerable. Patient satisfaction with the vaginal regimen is high and the majority of patients state that they would use the misoprostol method for a future termination and would also recommend the method to others.
Additional Uses of Misoprostol
Misoprostol is used for a wide array of conditions including the prevention of NSAID-induced gastric ulcers. Misoprostol is also used for a variety of obstetric and gynecological health indications, including the induction of labor, cervical ripening, and second trimester abortion. Misoprostol is also effective in both preventing and treating postpartum hemorrhage and managing both incomplete and missed abortion. Because misoprostol is effective in managing incomplete abortion, the medication has become an integral part of post-abortion care.